I doubt that many people would expect to be reading about cancer in an infectious disease blog, and yet here you are. Could it really be that I’m about to tell you that cancer, one of the most feared diseases in the developed world, can be contagious?
The answer is yes. That said, you don’t need to panic about a Hollywood-style infectious cancer outbreak just yet. Although there are examples of human cancers accidentally being transplanted into a new individual (1), these are rare and barely deserve being described as ‘infectious’. It could of course be argued that there are many viruses which can cause cancer (in fact, infectious agents are thought to cause 16.1% of cancers!), for example human papilloma virus which causes over 90% of cases of cervical cancers (2). However, in this case I am talking about cancers which are infectious in themselves.
The unfortunate animals affected are the cute-yet-ferocious tasmanian devils. Now only found on the island of Tasmania (an Australian state to the south of the mainland), the population of these carnivorous mammals has become endangered with thanks to a rampant infectious facial tumour. The cancer is transmitted between individuals when they fight over food. The tumour grows and eventually prevents them from eating, starving them. For a long time it was not undertood how the cancer was able to spread – normally the immune system would recognise the cells that were from another individual and reject them (much like you often hear happening with transplants). What is different this time?
A healthy Tasmanian devil Credit: arndbergmann
All normal cells express a class of molecule (known as MHCs) which lets the immune system know when a pathogen is in the cell. They are also the molecules which allow the immune system to spot foreign tissue, and are thereby the cause of transplant rejection. However, the cancerous cells don’t express these molecules, and so the immune system doesn’t respond to them (3). This means that when cancerous cells rub off onto another devil’s face, they are able to enter scratches and cuts and grow without being attacked by the immune system. Thankfully human cells are killed if they lack MHCs, so this should never evolve in human cancers.
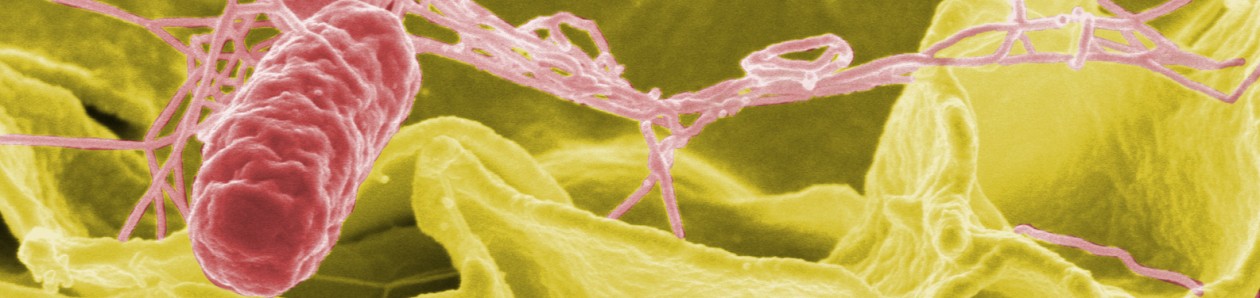
H1N1, H3N2, H1N7; we hear their names daily, but have you ever wondered what they mean? Why do we refer to the different strains of influenza by a ‘H’ and ‘N’ followed by a series of seemingly random numbers?
In order to replicate (reproduction is the ultimate ‘aim’ of all organisms!), viruses must first enter a host’s cell. In order to achieve this the virus must first interact with molecules on the host’s surface. These molecules must fit together like a lock and a key. If either one is the wrong shape, the virus won’t be able to enter the cell. As I described in ‘MERS CoV – will the Time-Bomb Explode?‘, this is especially important when looking at viruses which evolve to infect new species.
The letter ‘H’ stands for haemagglutinin, the ‘key’ on the virus. It binds to the ‘lock’ on the host cell, a molecule called sialic acid, and then enters. Interestingly, sialic acid is only found on animal lung cells, which is why we must inhale the virus to become infected!
The letter ‘N’ stands for neuraminidase. This is the ‘key’ which lets the virus back out of the cell. The virus needs to exit again so that it can go on to infect the next cell!
The haemagglutinin and neuraminidase proteins can vary, and each strain of virus will have one type of each. The number of each has been allocated purely based on the order in which it was discovered, so H1N1 has the first haemagglutinin and first neuraminidase proteins to be discovered.
That’s all very well, but why name a virus after these two proteins? The reason is that these proteins are the proteins that can most easily be ‘seen’ by the host’s immune system. Antibodies are made against these proteins, and this is what allows for the creation of immunity. That’s why being infected with H2N7 won’t protect you against H3N2 infection, and why scientists have to make informed guesses as to which strains should be vaccinated against in any one year.
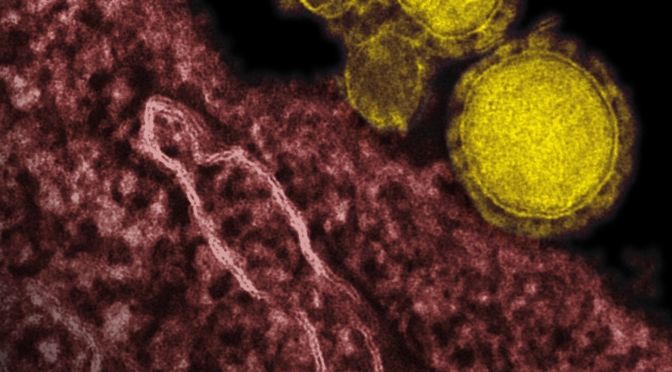
Transmission Electron Micrograph of MERS-CoV. Credit: NIAID
Over the last few weeks, the media have been particularly interested in covering the Ebola outbreak in West Africa (see my previous post, ‘Ebola – Time to Panic?‘), and this has resulted in rumours and scares about it spreading slightly closer to home. However, in my opinion, there is a virus which the developed world should be considerably more concerned about.
Middle East Respiratory Syndrome Coronavirus (MERS-CoV) is a virus very similar to the virus which caused the Severe Acute Respiratory Syndrome (SARS) outbreak in 2002/3, which resulted in 8,273 confirmed cases in 37 different countries, killing 775 (9%) (1). As the name suggests (scientists can be an incredibly imaginative bunch), MERS-CoV has been circulating mainly in Middle Eastern regions, including the Kingdom of Saudi Arabia, Qatar, and the United Arab Emirates (UAE) (2). The World Health Organisation (WHO) received reports of 254 laboratory-confirmed cases of MERS-CoV infection between September 2012 and the 24th of April, including 93 deaths (a fatality rate of over 35%)(3). There have been confirmed cases in people travelling to the Arabian Peninsula who have then brought the disease back to their home countries, in cluding the United Kingdom, France and, most recently, the USA, although no further infection is thought to have come from these (4). Symptoms include cough, fever, and shortness of breath (5), although there have also been links with side-effects such as stillbirths (6). There is currently no vaccine.
To understand these viruses a little better, we’re going to have to delve into their biology. Both MERS-CoV and SARS-CoV have genetic material made of a molecule known as RNA (ribonucleic acid). This is a molecule like DNA (deoxyribonucleic acid – our own genetic material), but it is less stable and more prone to mutation. This increased likelihood of mutation can be bad for the virus (much like mutations can be bad for humans), but some mutations will change the virus in a way which might make it more successful or able to do new things.
This mutation is important because both SARS-CoV and MERS-CoV are zoonotic viruses (transmitted from animals to humans) thought to originate in bats. However, the strain of the viruses found in bats are actually unable to infect humans. This is because the virus needs to be able to bind to certain molecules which vary between host species; think of a lock and a key – a key (virus molecules) to one door (host cells) will not open another (i.e. a different host species). However, by mutating the virus can change to allow it to bind the human molecules, and therefore infect humans – the key has changed to fit a new lock (although it probably can’t infect bats anymore!).
However, it is likely that a single mutation is not enough for the virus to be transmitted directly to humans (in this case think of the locks being so different that the keys have to change twice). This means that it is likely that there was an intermediate step, something where the locks are similar to both bats and humans which can act as a stepping stone. It has been suggested that SARS was passed from bats to civets (small carnivorous mammals), where it mutated again into a form able to infect humans (7). In a similar fashion, it is thought that camels act as a similar intermediate between the bat reservoir and human population for MERS-CoV.
Thankfully, although now able to infect humans, MERS-CoV is not well enough adapted to humans to be transmitted between humans multiple times. This is very similar to what we’ve seen before with different influenza strains, like bird flu. Although transmission may be possible, on average each infected person will infect less than one other person, meaning that the outbreak will die-out. However, the more people that are infected, the higher the chances that the virus will adapt to be spread between humans. If this happens, the average number of new infections from an infected individual may become greater than one – and then the virus will spread through the population.
It’s important to point out at this point that the virus doesn’t ‘want’ or ‘try’ to mutate – mutations are random events. Think of it in exactly the same way as animal evolution because exactly the same processes are involved; mutations are most likely to be deleterious, but once in a while they’ll make the individual more successful. The giraffe ancestors didn’t ‘want’ to grow longer necks, and lions didn’t ‘try’ to grow sharp teeth, random mutations slowly made these changes which made the individuals more successful. Remember, evolution is all about the survival of the fittest. It’s exactly the same with the virus – there’s no intention or fore-thought, but if it does evolve to infect humans, it has a whole new range of hosts it can infect!
So, should we be worried? As noted in the introduction, this virus almost certainly poses more of a threat globally than Ebola. My reasoning for this assertion lies within the routes of transmission – Ebola requires direct contact in order to spread, while MERS-CoV is thought to spread via droplets. At the moment, MERS-CoV is poorly adapted to humans, and so the only instances of transmission so far have been following lengthy contact with ill individuals, with small clusters within hospitals (8). However, as discussed above, there is the continual threat that it will become better adapted, and better at spreading. The question is, will it? The very nature of mutation is unpredictable, but the odds are probably in our favour (look at the history of these scares – there were more near-misses than real pandemics). That said, no one can truly say. Indeed, MERS-CoV may well be the time-bomb that we fear.
Amongst all of the uncertainty, what is certain is that if MERS-CoV doesn’t prove to be a global threat, there will soon be another virus which emerges to replace it. We must increase surveillance of potential reservoirs of these viruses, such as bats, so that we can better predict and prepare for the next outbreak. In my next post I shall address how we should go about this surveillance, whether or not we can predict the mutations required for human transmission of these viruses, and the biosecurity issues surrounding such research.
Colourised transmission electron micrograph of a Ebola Virus Virion. This media comes from the Centers for Disease Control and Prevention’s Public Health Image Library (PHIL), with identification number #10816
Science and health blogs are going wild. An Ebola epidemic originating in Guédeckou in southern Guinea, West Africa, is causing concern even for those many thousands of miles away. Why is this outbreak any different to the 14 other outbreaks that have occurred since the beginning of the new millenium? Is it true that the outbreak has reached Italy? Should we be worried? I’d like to think that I can help shed some light on each of these questions.
Before I dive into any speculation, it’s worth spending a moment to bring everyone up to speed about Ebola. As the name suggests, Ebola virus disease (EVD) is caused by the Ebola virus (1). Advanced symptoms of infection include vomiting, diarrhoea, and in some individuals, internal and external bleeding. This usually results in organ failure and severe dehydration, and can be fatal in up to 90% of cases.
The fatality rate of a disease isn’t the only important consideration when thinking about infectious disease – pathogens have evolved to maximise their transmission, and understanding how this occurs is essential for controlling their spread. Unfortunately, the prediction and control of the spread of Ebola is complicated by a current lack of understanding about how Ebola spreads in non-human hosts. The natural reservoir (long-term host where most of the viral population can be found) is believed to be various species of fruit bat which could be responsible for introducing Ebola to the area, although no transmission event to humans has ever been proven (2). The virus has also been shown to be carried by macaque monkeys (Philippines), and asymptomatically in pigs (Philippines and People’s Republic of China).
With regard to human-to-human transmission, Ebola virus is incredibly contagious. The virus infects new hosts via mucous membranes (e.g. mouth, urogenital tracts), across broken skin, or via contact with infected blood. However, once an outbreak has been identified, the necessity for direct contact makes control of the disease considerably easier than airborne diseases, despite the fact that symptoms may not appear for up to 21 days post-infection. Close monitoring must continue even after a patient appears to have recovered because they may remain infectious for up to 7 weeks after losing any symptoms. Unfortunately there is currently no vaccine or drug therapy available, making control of the outbreak incredibly difficult.
The current outbreak probably originated in Guinea many weeks prior to first World Health Organisation (WHO) notification on the 23rd of March which reported 49 cases and 29 deaths (3). Almost one month down the line, the WHO have reported 208 cases and 136 deaths in Guinea, including those of 16 healthworkers (4). This may seem alarming, but you only need to look back to 2007 to find a larger outbreak in the Democratic Republic of Congo (1). So why has this outbreak received so much attention?
An interview in the Independent suggests that the geographic spread of Ebola observed in Guinea is previously unprecedented, affecting a number of different towns, and even reaching across international borders into Liberia where there have been an additional 34 suspected cases (4, 5). This larger than normal coverage may be for a number of reasons. Firstly, there have never previously been any confirmed cases of the disease in Guinea, meaning that the local population are generally either unsure how to respond, or suspicious of the aid workers. Many believe that the health care workers actually harm their patients within their camps and have been blamed for bringing the disease to Guinea with them. Not only have the health workers been actively avoided by infected individuals, but violence has erupted in the Guniean city of Macenta against them (6).
However, the spread of cases into neighbouring Liberia is a far cry from recent rumours of cases in the southern Italian city of Pisa. Although by no means the source, the furthest back that I have been able to track the rumour is to Turner Radio Network, at which point I have been unable to find any further references (7). The website claimed that the virus was introduced to Italy by “40 illegal alien migrant workers“, and that “a statistical probability expert” has predicted that by the time we reach the 70th day of the outbreak the virus will have spread sufficiently that “nearly every place on the globe within 1000 miles of a commercial airport is fair game“. The article then goes on to describe how individuals should best prepare for a global pandemic.
Even if Ebola virus has reached Italy (which I doubt – see below), it is unlikely to spread in western culture. Many of the contributing factors to the spread of the disease in Guinea are irrelevant in more developed countries where healthcare workers are (generally!) respected, ill people seek help (and are more easily traced), and the dead are not touched.
To conclude this post, please allow me a small digression. While I can’t discount that the aforementioned article may be based on truth, I would argue that there are indicators that suggest that the article may not be entirely reliable, and could exhibit a degree of bias. Take from this carefully worded statement what you will, but I would always caution bloggers and readers from swallowing anything that isn’t supported by references or data, especially when something so newsworthy isn’t pounced on by other forms of media. Consider whether an author gains anything from spreading rumours (increased readership, support for a given cause, etc.) and generally consider the reputation of the author or publication. If we do not critically assess what we are reading, it is easy to disseminate false information as rumours that spread faster than the disease itself.
Infectious diseases are by no means glamorous subjects of conversation; most people avoid the topic like the plague (I’m sorry, I can be partial to the odd pun), and yet infectious disease is quite possibly the most fascinating area of all life sciences. The aim of this blog is to convince anyone who will listen that this is indeed the case.
This is where I hit my first hurdle – ‘anyone’ is a rather large potential audience, and it’s clearly impossible to write a post to suit everyone’s level of understanding at once. However, I’ll do my best to write a variety of posts so that everyone from the biologically uninitiated (my dad will be a good proof-reader for these!) to the most intense of professors will be able to find something that they enjoy.
I also intend to cover a range of subjects, from focussing on an individual pathogen of interest to discussing current disease outbreaks. If you have any topics that you’d like covered, let me know. Equally, if you have any questions along the way, get in touch – I can’t guarantee to be able to answer them all, but being a PhD student at one of the best univeristies in the world, it’s safe to say that I can find someone who can!